

Chances are you have met someone who has experienced injury at the local crag. Whether it is someone taping their fingers together to protect a “flexor pulley” at Smith Rock, cross-training at our neighbor’s Movement Gym in Portland, Oregon, to support their shoulder that has seen one too many dynos, or using belay glasses to protect their neck. The physical challenges climbing can place on your body are present in every move but can make a difference long after you’re done on the wall.
This blog is one of a series that will review the current research and training disciplines to delve into the most common climbing-related injuries and how to prevent them. Follow along to learn more about risk management and connect to resources that can keep you sending longer.
Overview
Injuries can occur for a multitude of reasons and are influenced by a web of factors, both controllable and not. These factors can include the duration and intensity of work on your body, the strength of your muscles, and the mobility of your joints. The determination of an injury can come from just the right combination of factors and how they prepare you for the climbing problem ahead of you.
One of the most recent climbing injury research reviews used eight independent studies to find the average incidence of injury to be 2.71 injuries per 1000 hours climbed (standard deviation +/- 4.49 injuries).1 These findings included results across all climbing disciplines and all ability levels.
The most common of these injuries reported rank in this order:1
- Flexor Pulley Injury
- Shoulder injuries
- Stress fractures of fingers in adolescents
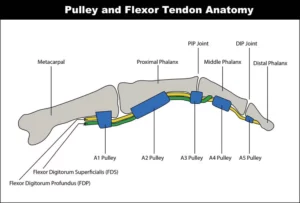
Annular Pulley Injuries, AKA Flexor Pulley Injuries
These are the most common and well-known climbing injuries, and they occur when the connective tissue holding the finger flexor tendons to the palm side of your hand strain or tear.2 A common cause of this is often a sudden, forceful loading (think, landing a dyno). People often experience an audible “pop” and have immediate pain and/or weakness. Another probable cause can be related to chronic degeneration with age and overuse.
(DeStefano, M. Pulley injuries explained – part 1. The Climbing Doctor. https://theclimbingdoctor.com/pulley-injuries-explained-part-1/ )
Conservatively, these injuries are treated based on the severity of the strain. With this information, a physical therapist can prescribe controlled rest, appropriate strengthening of the surrounding tissues, and a gradual return to activity. In terms of a complete rupture, a surgical consult may be necessary; in this case, a physical therapist will again guide the patient using similar principles once post-surgical rehab commences.
Shoulder Injuries
The shoulder is a complex system of four joints, and injuries can occur with the many interactions between its active and passive anatomical structures. Studies show shoulder injuries are positively related to the frequency and difficulty of sport climbing and bouldering, making up approximately 17% of climbing-related injuries.3 Among these injuries, the most commonly diagnosed are superior labral anterior-posterior (SLAP) tears and subacromial impingement (also known as subacromial pain syndrome).

(Slap lesion of the shoulder joint. Saint Luke’s Health System. (n.d.) https://www.saintlukeskc.org/health-library/slap-lesion-shoulder-joint)
The cause of these injuries can range from gradual to traumatic. Performance-wise, injuries can be connected to the repetitive overhead hanging and pulling motions required in the sport. Trauma-wise, landing dynos with a bent arm or falling back on an outstretched arm can all lead to sudden joint damage.4
Treatment of shoulder pain can be successful with proper attention to mobility, strength, and warm-up/cool-down principles. However, persistent or traumatic pain may require a diagnosis from a physical therapist or another appropriate medical professional to guide recovery.
Epiphyseal/Growth Plate Fractures of the Fingers in Adolescents
As the average age of competitive climbers decreases, the rate of injuries among youth increases. The most common of these injuries is a stress fracture to the growth plate within the climber’s finger.

(Erikson, D. L. (2015, December 12). Growth Plate fractures part 2. Finger Injury Help. https://www.climbinginjuriessolved.com/single-post/2015/12/12/growth-plate-fractures-part-2 )
These fractures are most often found in the middle or ring finger and can present with swelling and pain to the first knuckle (also known as the proximal Interphalangeal joint or PIP joint). The cause is tied to repetitive stress and loading of these bones/joints that are still growing.7
Young athletes have the advantage of growing faster than bamboo for their recovery. However, these injuries heal best when identified and managed early because they relate to these growth plate zones. At home, proper rest, sleep, and nutrition can be enough to calm down the joints and reduce pain. However, if the pain persists, it is recommended to receive a treatment plan from a rehab specialist to prevent stunted finger growth and persistent issues. A physical therapist will guide this process with controlled activity levels, education on healthy training discipline, and targeted strengthening to optimize a healthy return to sport.
What can be done?
If you ask any climber, climbing is about risk management. Whether using the proper belay system, having spotters move a crash pad mid-climb, or training responsibly, injury prevention is an ongoing process rather than a given.
The difference between these three practices is the active training and guidance provided. Any beginner will be provided courses for fall-related risk reduction. Few climbers will have the time or access to education about non-fall-related injuries or preventative training techniques.
Follow along with this series as we delve further into climbing-related injuries and preventative topics. The goal is to connect you with virtual resources to help build your toolbox and reduce the risk of injury.
Should you need more guidance, additional consultations and treatment are available from your neighborhood physical therapists at Rose City Physical Therapy, who specialize in climbing injuries and are also climbers. Schedule an appointment today!
Citations
- Jones, G. Schoffl, V. Johnson, M. (2018). Incidence, Diagnosis, and Management of Injury in Sport Climbing and Bouldering: A Critical Review. Current Sports Medicine Reports. 17(11):p 396-401. DOI: 10.1249/JSR.0000000000000534
- Schöffl V, Popp D, Kupper T, Schöffl I. (2015) Injury trends in rock climbers: evaluation of a case series of 911 injuries between 2009 and 2012. Wilderness Environ. Med. 26(1):62-7. doi: 10.1016/j.wem.2014.08.013.
- Chang CY, Torriani M, Huang AJ. (2016) Rock climbing injuries: acute and chronic repetitive trauma. Curr. Probl. Diagn. Radiol. 45:205–14. doi: 10.1067/j.cpradiol.2015.07.003.
- Popp D, Schöffl V. (2015) Superior labral anterior posterior lesions of the shoulder: current diagnostic and therapeutic standards. World J. Orthop. 6:660–71. doi: 10.5312/wjo.v6.i9.660..
- Schöffl V, Lutter C, Woollings K, Schöffl I. Pediatric and adolescent injury in rock climbing. Res. Sports Med. 2018; 26(Suppl. 1):91–113. doi: 10.1080/15438627.2018.1438278
- Jones G, Johnson MI. (2016) A critical review of the incidence and risk factors for finger injuries in rock climbing. Curr. Sports Med. Rep. 15:400–9. doi: 10.1249/JSR.0000000000000304.
- Schöffl I, Schöffl V. Epiphyseal stress fractures in the fingers of adolescents: biomechanics, pathomechanism, and risk factors. Eur. J. Sports Med. 2015; 3:27–37.
- DeStefano, M. Pulley injuries explained – part 1. The Climbing Doctor. https://theclimbingdoctor.com/pulley-injuries-explained-part-1/
Disclaimer: The content here is designed for information and education purposes only and is not intended for medical advice.